A journey of challenges with medication reconciliation
View File(s)
Session presented on Saturday, November 7, 2015 and Sunday, November 8, 2015:
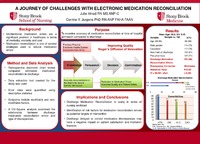
Background: Unintentional medication errors are a significant problem in healthcare in terms of morbidity, mortality and cost. Hospitalized patients are at particular risk for unintentional medication errors. At least 1.5 million Americans are injured every year by medication errors (IOM, 2006). On average, every hospital patient is likely subjected to at least one medication error per day, leading to approximately 98,000 annual deaths. Furthermore, the cost of medication errors is high in terms of negative patient outcomes and litigation. Over 3 billion dollars are spent annually towards treating the consequences of medication errors. Medication reconciliation is one of several strategies used to reduce medication errors. Medication reconciliation is the process of comparing a patient's medication regimen across the continuum by reviewing, analyzing and resolving any discrepancies.
Purpose: To examine the accuracy of electronic medication reconciliation upon admission compared to discharge. Theoretical Framework: One strategy to improve quality and prevent medication errors is to properly conduct medication reconciliation. Proper medication reconciliation is collection of a detailed medication history with open-ended questions, accurate documentation of medication reconciliation, and congruence with electronic technology. Changing processes supporting medication reconciliation is a challenge for healthcare systems. Rogers' theory of Diffusion of Innovations informs the process of change and adoption of improved medication reconciliation systems.
Review of Literature: Medication reconciliation emphasizes evaluating and improving medication regimen throughout the continuum to reduce patient harm. Few investigators have studied medication discrepancies on admission to discharge using electronic medication reconciliation. Patient safety is a challenge pertaining to preventing unintentional medication errors. Recent studies demonstrated that pharmacist- enhanced medication reconciliation improved patient outcomes, safety and reduced healthcare costs. Evidence supports using medication reconciliation processes to prevent medication errors. When nurses identified discrepancies, physicians changed the discharge orders of 94% of patients (Barnsteiner, 2005). Using electronic technology for medication reconciliation may generate a false sense of accuracy and security.
Method: A retrospective electronic chart review (n=200) was conducted at a tertiary care safety-net hospital, between July 2014 and December 2014 using a data extraction tool created for the study. Medication reconciliation conducted at admission and discharge was examined for medication discrepancies for patients admitted from the emergency department to cardiology and medical surgical units. Non-modifiable predisposing factors for medication reconciliation examined included age, gender, marital status, ethnicity, and comorbidities. Modifiable precipitating factors examined were medication discrepancies, change in medication regimen on discharge, polypharmacy, critical lab values and combination drugs. Variables were analyzed using descriptive statistics.
Results: The sample of 140 patients (mean age 58.8 years, SD 9.4) had more males than females and was predominately white. Preliminary results suggest that the prevalence of medication discrepancies were detected and corrected in greater than 50% of discharge medication reconciliations. More than 80% of patients were discharged home with a change in medication regime compared to their home regimen. Approximately 71% of patients reported to be on at least five medications or more. Most patients had comorbid illnesses; 86% had a history of hypertension; 67% had history of hyperlipidemia; 60% had a history of coronary artery disease.
Implications: Discharge Medication Reconciliation is costly in terms of nursing workload. Discrepancies detected during discharge medication reconciliation took approximately 30 minutes to correct. Delay in discharge to correct medication discrepancies may have a negative impact on patient satisfaction and financial management of the institution. Identification of risk factors for medication reconciliation serves as the potential targets of intervention. Outcomes rely on the health care provider's ability to identify risk factors and enter complete and accurate information in the electronic medical record.
43rd Biennial Convention 2015 Theme: Serve Locally, Transform Regionally, Lead Globally.`
Items submitted to a conference/event were evaluated/peer-reviewed at the time of abstract submission to the event. No other peer-review was provided prior to submission to the Henderson Repository, unless otherwise noted.
| Type | Poster |
| Acquisition | Proxy-submission |
| Review Type | None: Event Material, Invited Presentation |
| Format | Text-based Document |
| Evidence Level | N/A |
| Research Approach | N/A |
| Keywords | Medication Reconciliation; Medication Discrepancies |
| Name | 43rd Biennial Convention |
| Host | Sigma Theta Tau International |
| Location | Las Vegas, Nevada, USA |
| Date | 2015 |
All rights reserved by the author(s) and/or publisher(s) listed in this item record unless relinquished in whole or part by a rights notation or a Creative Commons License present in this item record.
All permission requests should be directed accordingly and not to the Sigma Repository.
All submitting authors or publishers have affirmed that when using material in their work where they do not own copyright, they have obtained permission of the copyright holder prior to submission and the rights holder has been acknowledged as necessary.
Related items
Showing items related by title, author, creator and subjects.
-
A journey of challenges with medication reconciliation
(2015-10-09)Background and purpose: Unintentional medication errors are a significant problem in terms of morbidity, mortality and cost. Medication reconciliation is one of several strategies to reduce medication errors. The purpose ... -
Improving medication safety through medication reconciliation in amulatory care
Background/Significance. Medication reconciliation (MR) is recognized as an effective strategy to prevent harm from medications and yet it has not been consistently performed in the ambulatory care setting. Inaccuracies ... -
Medication reconciliation: It's in the bag
(2016-03-21)Session presented on Monday, November 9, 2015: Background: Medication discrepancies, defined as unexplained differences in documented medications between various sites of care, occur in 70% of patients at hospital admission ... -
Improving medication adherence in the geriatric population with hypertension by using a teamlet model with a systematic program of medication reconciliation in a primary setting
(2016-03-17)Session presented on Sunday, July 26, 2015: This scholarly project examines one way to improve medication adherence among elderly patients diagnosed with hypertension by educating clinical staff on the teamlet model. ... -
Development of a medication reconciliation policy in outpatient mental health facility
Introduction/Background: Adverse drug events and medication discrepancies are patient safety challenges for patients and healthcare professionals. Medication errors result in approximately 7000 deaths annually, and adverse ...




